Medication Safety for Caregivers: How to Protect Loved Ones from Dangerous Errors
Every year, over 1.5 million people in the U.S. are harmed by medication errors - and most of them happen at home, not in hospitals. If you’re caring for an aging parent, a child with special needs, or someone with chronic illness, you’re likely managing multiple pills, liquids, patches, and injections. One wrong dose, one missed schedule, or one misunderstood instruction can lead to a hospital trip - or worse. The good news? Most of these errors are preventable. With clear steps, simple tools, and a few smart habits, you can turn medication management from a source of stress into a reliable routine.
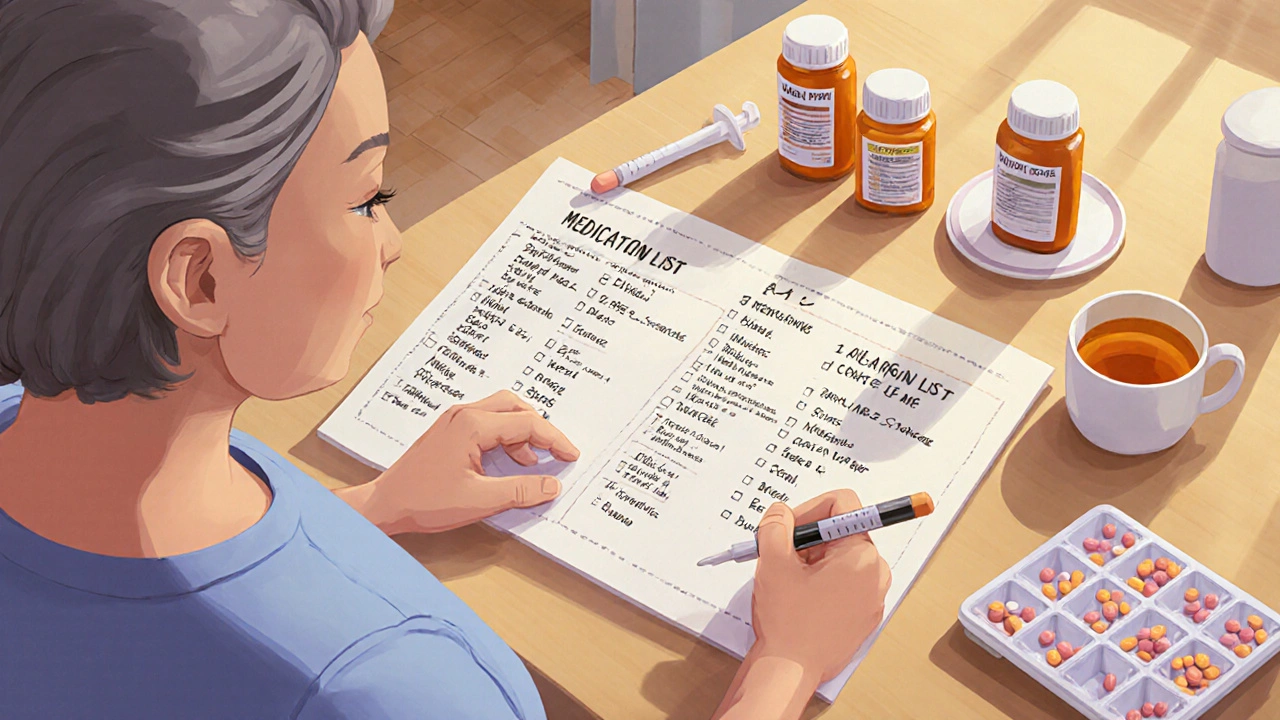
Start with a Complete Medication List
You can’t manage what you can’t see. The first step to safety is creating a real, up-to-date list of every medication your loved one takes. This isn’t just a mental note or a scribble on a napkin. It needs to include:- Brand name and generic name (e.g., Lipitor and atorvastatin)
- Exact dosage (e.g., 10 mg tablet, 5 mL liquid)
- How often it’s taken (e.g., once daily at bedtime, every 6 hours as needed)
- Why it’s prescribed (e.g., “for high blood pressure,” “for sleep”)
- Any side effects you’ve noticed
Doctors and pharmacists don’t always know everything your loved one is taking - especially over-the-counter drugs like ibuprofen, antacids, or herbal supplements. A 2021 study in Mayo Clinic Proceedings found that caregivers who kept a full list reduced medication errors by 52%. Start with a blank sheet of paper. Call the pharmacy. Check the original bottles. Ask the doctor. Take 60 to 90 minutes once to get it right. Then update it every time something changes.
Watch Out for Polypharmacy and High-Risk Drugs
Taking five or more medications at once - called polypharmacy - increases the risk of harmful side effects by 88% in adults over 65, according to the Agency for Healthcare Research and Quality. Many of these drugs aren’t even necessary. A 2021 New England Journal of Medicine study found that nearly half of older adults are taking at least one drug that does more harm than good.Two of the most common culprits:
- Proton pump inhibitors (PPIs) - like omeprazole - often prescribed for heartburn, but used for years without review. Long-term use can cause kidney damage, bone loss, and nutrient deficiencies.
- Benzodiazepines - like lorazepam or diazepam - used for anxiety or sleep, but increase fall risk and confusion in older adults.
The Beers Criteria, updated annually by the American Geriatrics Society, lists 30 medications that should generally be avoided in seniors. Bring your medication list to every doctor visit and ask: “Is this still needed? Are there safer alternatives?” Don’t be afraid to say, “Let’s try stopping this one.”
Use the Right Tools - No Guesswork
Household spoons are dangerous. A 2021 JAMA Pediatrics study showed they can deliver 20% to 40% more or less medicine than intended. Always use the measuring device that comes with the bottle - usually a calibrated oral syringe or dosing cup. Keep it with the medication. Never substitute.For people with memory issues, a seven-day pill organizer with AM/PM compartments is essential. The Alzheimer’s Association recommends them for anyone with dementia. But don’t just dump pills in - check the list first. Some pills shouldn’t be split, crushed, or opened. Talk to the pharmacist about which ones are safe to put in the organizer.
Alarms help, too. Many pill organizers now have built-in alarms. Or use a simple phone alarm labeled “Morning Pills” or “Evening Blood Pressure.” One caregiver on ALZConnected said her mom went from missing 4 doses a week to zero after setting three daily alarms on her tablet.
Store Medications Correctly
Medications aren’t like cereal - they don’t last forever, and they don’t like heat or moisture. The FDA recommends storing most pills and liquids between 68°F and 77°F (20°C to 25°C). That means no more medicine in the bathroom cabinet, where steam from showers ruins them. Keep them in a cool, dry drawer or shelf.Check expiration dates every week. It takes 10 minutes. A 2023 FDA report found that 90% of caregivers don’t regularly check. Expired antibiotics can lose effectiveness. Old insulin can stop working. Out-of-date liquid pain relievers can grow bacteria. Throw out anything past its date - don’t wait for “just in case.”
Get Help from the Pharmacist
Pharmacists are medication experts - not just people who hand out pills. Yet most caregivers never ask them for help. In 2022, the American Pharmacists Association found that pharmacists caught potential problems in 35% of visits where caregivers asked questions.Request a Medication Therapy Management (MTM) review. It’s free if your loved one is on Medicare Part D and takes 8 or more medications. The pharmacist will review everything - check for duplicates, dangerous interactions, and unnecessary drugs. One caregiver shared on FamilyCaregiver.org: “After my MTM review, the pharmacist found three interactions I didn’t know about. Two of those pills were causing my dad’s dizziness.”
Ask for a medication reconciliation every time your loved one leaves the hospital. The CARE Act, now law in 47 states, requires hospitals to give this to caregivers before discharge. Don’t accept a discharge without it.
Use Technology - But Keep It Simple
Apps like Medisafe and CareZone send reminders, track doses, and let you share updates with other caregivers. A 2023 Caregiver Action Network survey found users reported 32% fewer missed doses than those using paper logs.But if your loved one or you are over 65, don’t force tech if it causes stress. A National Institute on Aging focus group found 27% of older caregivers felt overwhelmed by apps. If digital tools aren’t working, stick with paper lists, alarms, and pill organizers. The goal isn’t to be high-tech - it’s to be accurate.
Prepare for Transitions - The Most Dangerous Time
The biggest spike in medication errors happens when someone moves from hospital to home. A 2022 study by Dr. Joanne Lynn found 62% of errors occur during this transition. Hospitals change meds. Discharge papers are confusing. You get home and realize: “Wait - did they take off the blood thinner?”Before discharge, ask for a written plan: “What meds were stopped? What’s new? What’s the dose now?” Take the list to your pharmacist the same day. Don’t wait. If you’re unsure about a change, call the hospital pharmacy. It’s better to ask twice than to give the wrong pill.

Make It a Weekly Habit
Medication safety isn’t a one-time task. It’s a rhythm. Set aside 10 minutes every Sunday to:- Check expiration dates
- Count pills - are any missing or extra?
- Compare the list to what’s in the bottles
- Refill prescriptions early - don’t wait until you’re out
St. Jude Together Medical Care Center found this simple weekly check prevented 18% of potential errors in pediatric care. It works for adults too. A few minutes a week saves hours in the ER.
Know the Look-Alike, Sound-Alike Risks
Some drug names are dangerously similar. Hydroxyzine (for allergies) vs. hydrocortisone (for skin rashes). Clonidine (for blood pressure) vs. clonazepam (for seizures). The Institute for Safe Medication Practices says these mix-ups cause 15% of reported errors.Always read the label aloud before giving a pill. Say the full name: “Hydroxyzine - 10 mg - for itching.” Ask the pharmacist to flag high-risk drugs with a sticker. Many pharmacies now put red warning labels on these.
It’s Not Perfect - But It’s Manageable
You won’t catch every mistake. You’ll forget a dose sometimes. You’ll get confused. That’s normal. What matters is having systems in place so one slip doesn’t turn into a crisis.Medication safety isn’t about being perfect. It’s about being prepared. It’s about asking questions. It’s about trusting your gut - if something feels off, call the pharmacist. If the pill looks different, ask why. If the schedule is too complicated, say so.
Every year, 30% of hospital readmissions for older adults are caused by medication errors. You can change that. With a clear list, the right tools, and a little routine, you’re not just managing pills - you’re protecting someone you love.
What should I do if I think my loved one is taking too many medications?
Start by making a complete list of every pill, liquid, patch, and supplement they take. Then schedule a Medication Therapy Management (MTM) review with their pharmacist - it’s free if they’re on Medicare Part D. Bring the list to their doctor and ask: “Which of these are still necessary? Are there safer alternatives?” Don’t stop any meds on your own. Work with the team to reduce or replace high-risk drugs like benzodiazepines or long-term proton pump inhibitors.
Can I use a regular spoon to give liquid medicine?
No. Household spoons vary by 20% to 40% in volume, which means you could be giving too much or too little. Always use the measuring tool that came with the medicine - usually a calibrated oral syringe or dosing cup. Keep that tool with the bottle so you don’t lose it. If it’s missing, call the pharmacy for a free replacement.
How often should I check expiration dates?
Check every week. It takes less than 10 minutes. The FDA says 90% of caregivers don’t do this regularly, but expired medications can lose strength or become unsafe. Liquid antibiotics, insulin, and eye drops are especially risky after their expiration date. When in doubt, throw it out.
What’s the best way to help someone with dementia take their meds?
Use a seven-day pill organizer with AM and PM compartments. Set alarms on a phone or tablet. Never rely on memory. The Alzheimer’s Association recommends this as a standard practice. If they refuse to take pills, talk to their doctor - sometimes changing the form (like switching from a pill to a liquid) helps. Avoid hiding pills in food unless approved by a pharmacist - some meds can’t be crushed or mixed.
Is it safe to keep all medications in one place?
Yes - as long as it’s secure and away from heat and moisture. Store all medications together in a cool, dry drawer or cabinet, out of reach of children or pets. Don’t keep them in the bathroom or near the stove. Label the container clearly. This makes it easier to check doses, spot duplicates, and prevent accidents. Just make sure it’s locked if there’s a risk of misuse.
What should I do if my loved one misses a dose?
Don’t double the next dose unless the doctor says so. Call the pharmacist or doctor right away. For some meds - like blood thinners or insulin - missing a dose can be dangerous. For others - like antibiotics - it’s less urgent but still affects treatment. Keep a log of missed doses so you can report patterns. Use reminders to prevent future misses.
Are there free services to help with medication management?
Yes. If your loved one is on Medicare Part D and takes 8 or more medications, they qualify for free Medication Therapy Management (MTM) from their pharmacy. CVS and Walgreens now offer free prescription synchronization - all refills are due on the same day each week. The Caregiver Action Network also offers free online guides and webinars. Don’t pay for services that promise to manage meds - many free options exist.
How do I know if a medication is high-risk for older adults?
Look for the Beers Criteria list, which identifies 30 medications that are risky for seniors. Common ones include benzodiazepines (like Valium), anticholinergics (like diphenhydramine in Benadryl), and long-term NSAIDs. Pharmacists now often flag these with red stickers on bottles. Ask your pharmacist: “Is this on the Beers list?” If it is, ask if there’s a safer option.
ka modesto
November 28, 2025 AT 11:26Just started using a pill organizer with alarms after my dad missed his blood pressure med for three days straight. Game changer. Also made a list of everything he’s on-turned out he was taking two different versions of the same statin. Pharmacist caught it. No more panic Sundays.
Pro tip: write the reason next to each med. ‘For sleep’ or ‘for cholesterol’ helps when you’re half-asleep at 2 a.m. and holding a pill in your hand.
Holly Lowe
November 28, 2025 AT 19:59OMG YES. I used to throw meds in the bathroom like they were socks. Then my grandma’s insulin went bad and she ended up in the ER. Now everything lives in a locked drawer in the bedroom with a little fan blowing air in. It’s like a tiny medicine temple. And I check dates every Sunday like it’s my sacred duty. No more ‘eh, it’s probably fine’ vibes.
Also-stop using spoons. Just stop. I don’t care if your spoon is ‘kinda close.’ It’s not. Get the damn syringe.
Samantha Stonebraker
November 30, 2025 AT 19:10There’s something deeply human about this topic-it’s not just about pills and schedules, it’s about dignity, patience, and quiet love. We don’t talk enough about how exhausting this work is. You’re not just a caregiver-you’re a pharmacist, a detective, a translator, and sometimes, a grief counselor.
I used to feel guilty when I forgot a dose. Then I realized: perfection isn’t the goal. Systems are. A checklist. A reminder. A calm voice asking, ‘Is this right?’ That’s the real magic. Not the flawless execution. The willingness to try again tomorrow.
And yes-pharmacists are unsung heroes. Talk to them. They’ve seen it all. They won’t judge you. They’ll help you.
Kevin Mustelier
December 1, 2025 AT 12:02Lmao. ‘Use a pill organizer.’ Sure. And then what? Your 87-year-old mom with dementia thinks it’s a toy and dumps it in the toilet. Or your dad starts hoarding expired Tylenol ‘just in case.’
Real talk: most of this advice is for people who still have their cognitive faculties. Try managing meds for someone who thinks the pills are spies. The ‘weekly check’? Cute. My aunt hides hers in her bra. No, I’m not kidding.
Maybe stop pretending this is a checklist problem. It’s a human problem. And humans are messy. Always have been. Always will be.
Keith Avery
December 1, 2025 AT 18:26Let’s be real-the entire premise of this post is a middle-class fantasy. You assume everyone has access to a pharmacist who does MTM reviews, a tablet for alarms, a cool dry drawer, and the time to do a ‘weekly check.’
My cousin’s mom is on Medicaid in rural Alabama. She gets her meds delivered in a brown bag. The ‘dosing cup’? Never came with the bottle. The ‘Beers Criteria’? She doesn’t know what that is. And the doctor? He’s 120 miles away and only sees her once a year.
This isn’t ‘preventable errors.’ This is systemic neglect dressed up as a blog post. Good intentions don’t fix broken systems.
Luke Webster
December 2, 2025 AT 23:28I grew up in a family where meds were just… there. No labels. No lists. Just ‘take the white one in the morning.’ I didn’t realize how dangerous that was until my wife’s dad had a stroke from mixing ibuprofen and blood thinners.
What changed everything? We started talking. Not just about pills, but about fear. He was scared of being a burden. She was scared of making a mistake. Once we named those feelings, we could build systems around them-not just checklists, but compassion.
And yeah, sometimes the ‘right’ tool is a handwritten note taped to the fridge. Doesn’t have to be fancy. Just consistent.
Simran Mishra
December 4, 2025 AT 22:20Oh my god. I’ve been doing this for 7 years and I just want to cry. My mom has dementia and I’ve been giving her pills since 2017 and I swear sometimes I think I’m the only one who remembers she even takes them. I’ve had nights where I just sit in the kitchen holding the pill organizer and sob because I don’t know if I gave her the right one or if I already gave it or if she took it and spat it out or if the pharmacy gave me the wrong bottle and I’m so tired and no one understands how lonely this is and I’m scared I’m going to kill her by accident and I don’t even know what to do anymore.
I just… I just need someone to say it’s okay that I’m not perfect. That it’s okay that I cry. That I’m doing my best. And I know this post is supposed to help but I just… I just needed to say it out loud.
Thank you for writing this. Even if I’m not doing it right. Even if I’m failing. Thank you.
Orion Rentals
December 5, 2025 AT 17:08While the recommendations presented are commendable in intent, they presuppose a level of socioeconomic privilege and healthcare infrastructure that is not universally accessible. The notion of a ‘Medication Therapy Management’ review being ‘free’ under Medicare Part D is contingent upon eligibility criteria that exclude a significant portion of the aging population, particularly those without consistent access to primary care or pharmacy services. Furthermore, the reliance on digital tools such as Medisafe or CareZone assumes technological literacy and device ownership, which are not guaranteed in elderly populations. A more robust framework would integrate community-based health workers and mobile pharmacy units to bridge these disparities.
Sondra Johnson
December 6, 2025 AT 01:01Okay but let’s talk about the REAL villain here: Big Pharma. They push these high-risk meds like they’re selling candy. PPIs? Benzodiazepines? They’ve been marketing these for decades like they’re miracle cures. And then when people get sick from them, the docs just write another script.
I called my mom’s doctor and said, ‘Why is she still on this damn lorazepam?’ He said, ‘Oh, we’ve been meaning to wean her off.’ We’ve been meaning to? For THREE YEARS?
Stop blaming caregivers. Start holding doctors and drug companies accountable. We’re just trying not to kill our parents. They’re the ones selling the poison.
Chelsey Gonzales
December 7, 2025 AT 13:15im so bad at this i keep mixing up the blue pill and the green one and i think i gave my mom her blood pressure med at breakfast instead of bedtime and now i think she might be mad at me but she cant say so because of her stroke and i just cry every night and feel like the worst daughter ever
also i use a spoon sometimes but i only do it when im in a rush and i swear i measure it with my eye and its like… kinda right??
MaKayla Ryan
December 8, 2025 AT 17:57This is why America is falling apart. You let some 65-year-old woman with no medical training manage insulin and blood thinners? That’s not ‘care,’ that’s negligence. Someone should be licensed to give meds. Like a pilot. Or a surgeon. Not some stressed-out daughter using a kitchen spoon.
Stop glorifying ‘just doing your best.’ That’s not good enough. We need rules. Laws. Penalties. This isn’t a blog post. It’s a public health emergency.
Kelly Yanke Deltener
December 9, 2025 AT 23:43I’m so tired. I’ve been doing this for 5 years. My mom’s on 14 meds. I’ve lost 20 pounds. I don’t sleep. I cry every night. I’m 38 and I feel 80.
And everyone says, ‘Oh, you’re such a good daughter!’
What no one says is: ‘You’re drowning.’
And the system? It doesn’t care. The pharmacist doesn’t call. The doctor doesn’t answer. The government doesn’t fund respite care.
I’m not a hero. I’m just someone who hasn’t broken yet.
Thank you for this post. I needed to feel seen.
Crystal Markowski
December 10, 2025 AT 20:54The implementation of structured medication reconciliation protocols, particularly during care transitions, remains critically underutilized despite evidence demonstrating significant reductions in adverse drug events. The CARE Act, while a step forward, lacks standardized enforcement mechanisms across states. I recommend integrating automated electronic health record alerts triggered by polypharmacy flags, coupled with mandatory pharmacist-led discharge counseling. Furthermore, the use of barcode scanning at the point of administration-though underused in home settings-could dramatically reduce dosing errors. These are not aspirational ideals; they are scalable, evidence-based interventions requiring policy prioritization.
Charity Peters
December 11, 2025 AT 16:20My grandma just takes her pills with her coffee. No organizer. No list. Just ‘oh yeah, I take the little white one.’
She’s 92. She’s fine.
Maybe not everyone needs all this stuff.
Faye Woesthuis
December 12, 2025 AT 07:26If you can’t manage pills, don’t be a caregiver. That’s it. End of story. This isn’t a ‘heartfelt journey.’ It’s a job. And if you’re too lazy to use a measuring cup or check expiration dates, you shouldn’t be handling life-or-death meds. People die because of this carelessness. Stop making excuses.
ka modesto
December 12, 2025 AT 11:33Just saw someone say ‘my grandma’s fine without all this.’ I get it. My grandma was too. But she also had a stroke from a missed blood thinner dose at 89. She’s fine now… but she can’t talk. And she doesn’t remember what happened.
Some people get lucky. Others don’t. I’d rather be the one who checked the bottle.
Thanks for the reminder, everyone. We’re all doing the best we can.